Hip arthrolysis
You have hip impingement
You are going to undergo hip arthrolysis
You have hip impingement
You are going to undergo hip arthrolysis
Hip arthrolysis
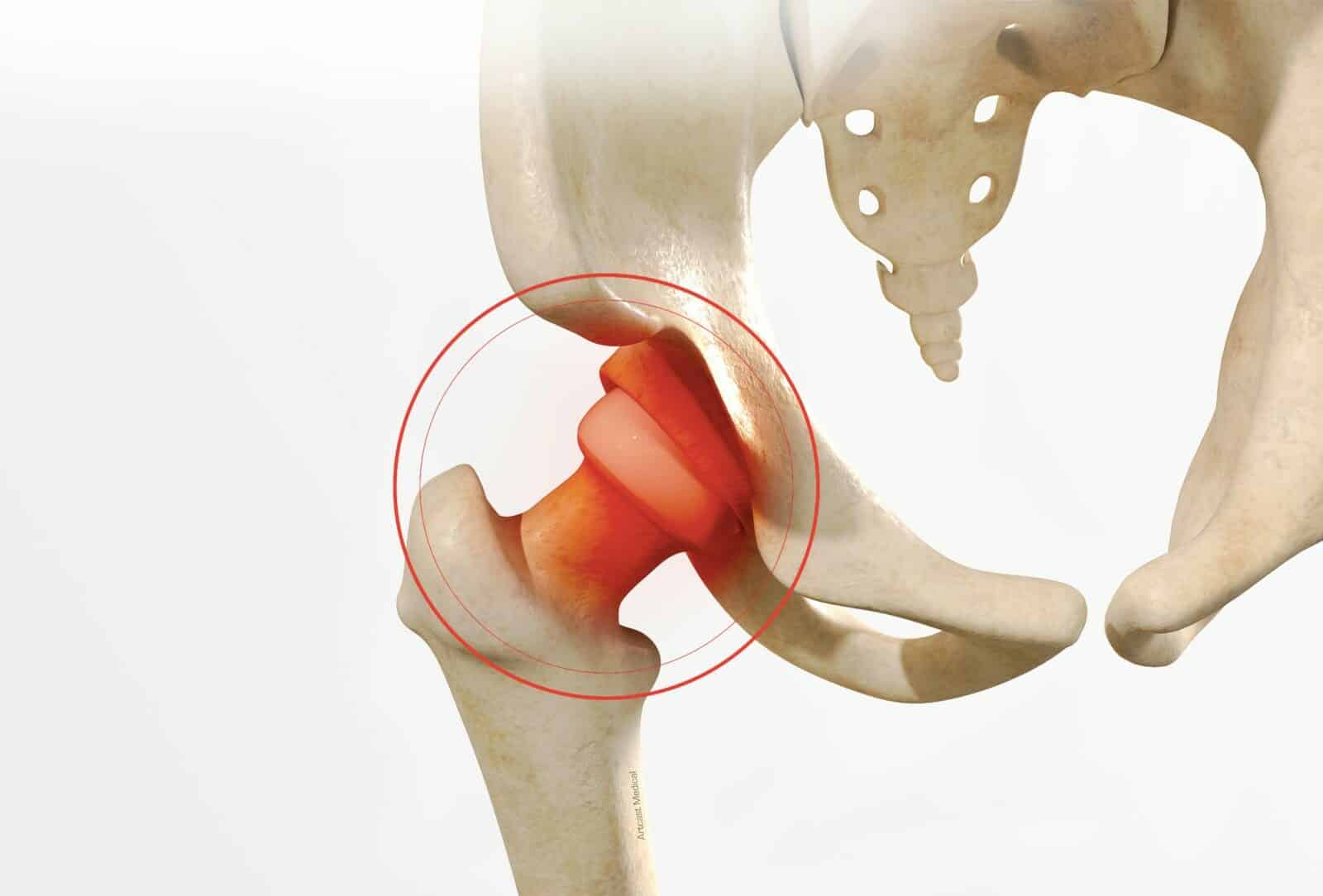
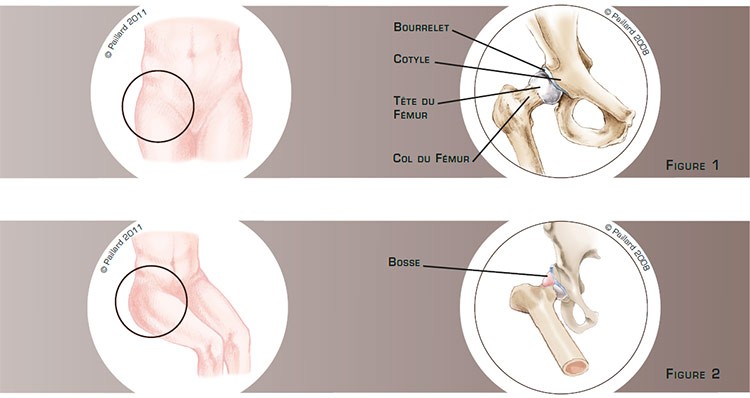
The hip is the joint between the pelvis and the femur. The top of the femur is composed of a head and a neck, which pivots in a socket in the pelvis called the acetabulum; the sliding surfaces are lined with cartilage. The labrum is a sort of C-shaped cushion, which improves the contact and acts as a shock absorber between the cartilage of the femoral head and the acetabulum (figure 1). Hip impingement is excessive contact between the femoral neck and the edge of the acetabulum. Certain sports, such as martial arts, dancing or athletics, as well as certain anomalies, such as a deformity on the anterior side of the neck or the rim of the acetabulum which sticks out too far, can cause this impingement during extreme movements of the hip. This repeated contact can thus damage the labrum and the cartilage (figure 2).
The impingement causes pain and restricts hip mobility. The discomfort is felt more when playing sports or when completely bending the hip.
With hip impingement it may not be possible to carry out some sports activities and some daily activities.
This impingement does not disappear spontaneously and will progressively damage the labrum and the cartilage. In this context, the natural progression is the gradual deterioration of the joint and therefore increased discomfort. The aim of arthrolysis is to recover normal, painless mobility so as to be able to carry out all types of activities, thus preventing labrum and cartilage damage and the deterioration of the joint.
Hip arthrolysis consists in eliminating the excessive contact between the femoral neck and the edge of the acetabulum.
On the femur, the bump on the anterior side of the neck is resected (figures 3 and 4).

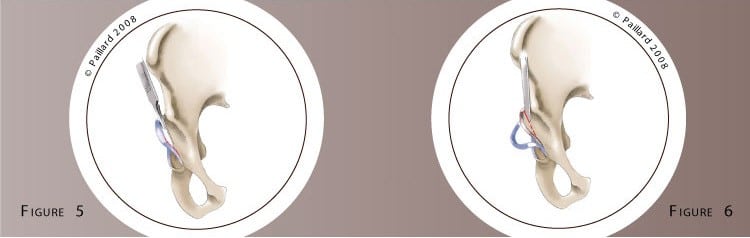
On the the acetabulum, after detaching the labrum (figure 5), the excess rim is trimmed (figure 6).
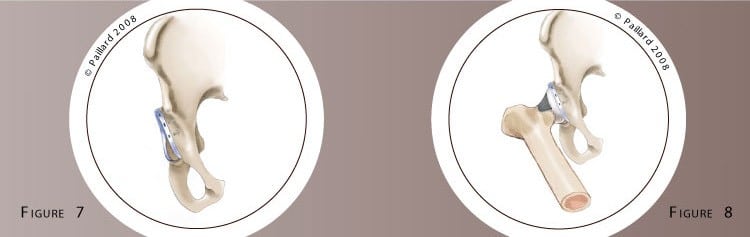
At the end of the operation, the labrum is reinserted (figure 7) and hip movement is controlled with extreme hip motions (figure 8). Morphological defects are more frequent on the femur than the acetabulum; the femoral procedure is systematic whereas that of the acetabulum is inconstant.
According to your morphology and the hip damage identified,
this procedure can be performed using an anterior approach or arthroscopically. If an arthroscopic technique is used, several small 5-mm incisions are made around the hip. An arthroscope, or small camera, is inserted through one of the incisions to view the joint. Small instruments are inserted through the other incisions to carry out the surgery. The anterior approach requires a short incision on the anterior of the hip. A passage is created between the various muscles by moving them aside to access the joint and treat the damage.
Even if we prefer arthroscopy as it is possible to access the joint without opening it, the anterior approach is often necessary. It does however spare the hip muscles and enables faster post-operative recovery.
The operation lasts about 1 hour on average, and requires around 3 days in hospital.
Total hip replacement is carried out under spinal or general anaesthesia. Your anaesthesiologist will decide with you the best type of anaesthesia according to your state of health.
After the operation, the incisions are covered with a sterile dressing, which is left in place for 10 days. The pain will be managed and monitored very closely during the post-operative period, and the treatment will be adjusted accordingly.
The day after the operation, the physiotherapist will get you up and help you to walk. Walking sticks will be useful during the first few days, but will be rapidly abandoned. In the case of a procedure on the acetabulum with reinsertion of the labrum, you will have crutches to help you move around for 4 weeks so as not to put too much weight on your hip. It is not necessary to go to a rehabilitation centre or see a physiotherapist after your stay in hospital. Progressively resuming your activities will be your physiotherapy.
Driving can be envisaged rapidly, and you can generally return to work after the 1st month, depending on your profession; office work can be sooner. You can progressively resume sports activities after the 3rd month, but it is often necessary to wait until the 6th month to return to competition.
In addition to the risks associated with any surgery and the anaesthetic, there are some risks specific to this surgery :
This list of risks is not exhaustive. Your surgeon can provide you with any additional explanations and will be available to discuss the advantages, disadvantages and risks of the operation with you.
The pain disappears and full mobility is recovered very rapidly after the operation.
This pathology has not been known for long, and so there are no long-term results available. However, we hope that the disappearance of the hip impingement will prevent labrum and cartilage damage and thus prevent the deterioration of the joint and the development of osteoarthritis.
The results of this technique are encouraging as an improvement in hip function is observed in over 90 % of cases and a return to sports activities in over 80 % of cases. Furthermore, the results are better if the surgical procedure is carried out before any serious damage to the cartilage occurs.
Laissez votre commentaire