Elbow arthrolysis
You suffer from elbow stiffness
You are going to undergo elbow arthrolysis
You suffer from elbow stiffness
You are going to undergo elbow arthrolysis
Elbow arthrolysis
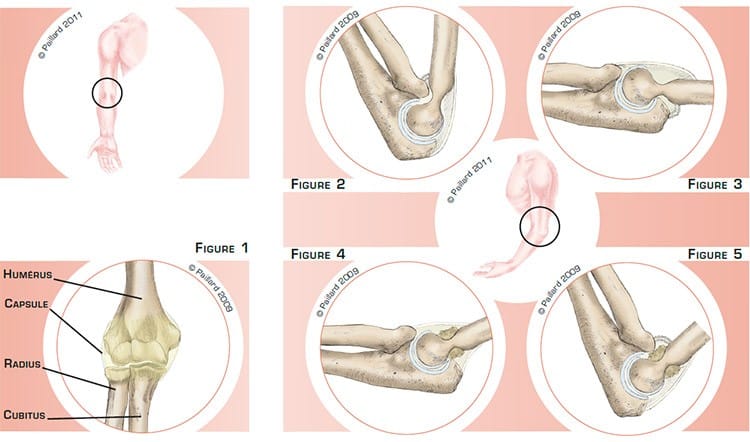
The elbow is the joint between the humerus, the cubitus and the radius (figure 1). There are processes and grooves so they fit together perfectly and enable full mobility. The inferior part of the humerus articulates with the superior part of the cubitus and the radius allowing the flexion (figure 2) and extension of the elbow (figure 3). The head of the radius articulates with the cubitus and can turn on itself to rotate the wrist. The sliding surfaces are lined with cartilage.
The joint is surrounded by a flexible, elastic envelope called the joint capsule. The anterior part stretches when you straighten your elbow until it is fully extended, and vice versa for the posterior capsule when you bend your elbow.
Numerous tendons attach the muscles to the bone surrounding this joint, in particular the biceps to bend the elbow and the triceps to straighten the elbow.
Elbow stiffness can occur suddenly after a trauma or a fracture, or it can develop progressively in the case of osteoarthritis. The capsule thus becomes stiffer, like a chamois leather, and prevents full mobility. The grooves in which the bones fit together can fill and form processes, thus limiting mobility.
This will lead to difficulties in flexing (figure 4) and bending the elbow (figure 5), and rotating the wrist, and cause discomfort for certain physical or daily activities.
Some sports or daily activities are not possible due to elbow stiffness. If the elbow is unresponsive after several months of appropriate rehabilitation, elbow arthrolysis is indicated.
The aim of the operation is to improve and even recover complete mobility, strength and function.
Elbow arthrolysis consists in removing the retracted capsule, the impinging bone and the adhesions around the head of the radius.
A short incision is made in the external part of the elbow. In some cases, an incision is also made on the inside.
The joint capsule is then exposed; the anterior part (figure 6) and the posterior part (figure 7) are excised using a scalpel.
A new, more flexible capsule will subsequently reform allowing recovery of normal joint function.

The bone processes are resected using a motorised cutter.
The normal lines of the humerus and cubitus are excavated so the bones fit together better (figures 8 and 9).
The adhesions around the head of the radius and the cubitus are removed to restore wrist rotation.
All these procedures help improve elbow mobility (figures 10 and 11).
In some cases, arthrolysis can be carried out arthroscopically, depending on your morphology, the damage diagnosed as well as surgical history.
An arthroscopy consists in making several small 5-mm incisions around the elbow. An arthroscope, or small camera, is inserted through one of the incisions to view the joint.
Small instruments are inserted through the other incisions to perform the surgery.
The operation lasts about one and a half hours, and requires around 5 days in hospital.
Elbow arthrolysis can be carried out under regional or general anaesthesia. Your anaesthesiologist will decide with you the best type of anaesthesia according to your state of health.
After the operation, the incisions are covered with a sterile dressing, which is left in place for 10 days. The pain will be managed and monitored very closely during the post-operative period, and the treatment will be adjusted accordingly.
As soon as you return to your room, your elbow will be placed in an arthromotor, a device that will continuously bend and straighten your elbow 24 hours a day to start with.
The physiotherapist will explain to you how the machine works. When you leave the clinic, you will take the arthromotor home with you and continue your rehabilitation for one month.
In the second month, more traditional rehabilitation will continue with your physiotherapist.
You will also be able to resume driving as well as sports activities that do not put any strain on the upper limb. You can generally return to work during the 2nd month, depending on your profession; office work can be sooner.
After the 3rd month, you can resume all physical and sports activities, with no restrictions.
In addition to the risks associated with any surgery and the anaesthetic, there are some risks specific to this surgery :
This list of risks is not exhaustive. Your surgeon can provide you with any additional explanations and will be available to discuss the advantages, disadvantages and risks of each specific case with you.
Mobility is recovered immediately after the operation. It is about 70 % of the initial deficit and very much depends on the quality of the postoperative rehabilitation. In the case of moderate stiffness, full recovery of mobility can be expected.
These results persist over time and revision surgery is rarely necessary.
The results of this technique are very encouraging as patient satisfaction and improvement in function are observed in over 90 % of cases.
Laissez votre commentaire