Meniscal surgery
You have meniscal damage
You are going to undergo meniscal surgery

You have meniscal damage
You are going to undergo meniscal surgery
Meniscal surgery
The knee is the joint between the bottom of the femur and the top of the tibia, and the sliding surfaces are lined with cartilage. The menisci are small C-shaped cushions between the cartilage of the femur and the tibia. There are two menisci in each knee: a medial and a lateral meniscus (figures 1 and 2).
The menisci are made of fibrocartilage. They improve the contact and act as shock absorbers between the femur and the tibia. Their function and consistence are reminiscent of plumbing washers. With time, the menisci tend to lose moisture and the cartilage gets thinner.
Meniscal damage can occur following a blow to the knee or recurrent minor traumas suffered during certain movements. This lesion can affect the meniscus to a varying extent. It can be stable (figure 3 and photo 1), or unstable in the form of a bell clapper that moves in the joint (figure 4 and photo 2).
This damage causes pain, locking, swelling and sometimes a feeling of instability of the knee. Cartilage damage can be associated with and participate in this painful symptomatology.

The menisci are poorly vascularized and do not heal well. An unstable lesion does not heal spontaneously and a small lesion can initially be treated medically. Surgery will be proposed in the case of unstable symptomatic meniscal damage or stable meniscal damage that is not relieved by medical treatment. The objective of the operation is to relieve the pain, locking and swelling, and enable a return to normal walking and activities.
Meniscal surgery is performed arthroscopically, without opening the joint. Arthroscopy consists in making two small 5-mm incisions in the front of the knee. An arthroscope, or small camera, is inserted through one of the incisions to view the joint, and in particular the damaged meniscus. Small instruments are inserted through the other incision to carry out the surgery. Two procedures can be envisaged according to the damage; we will try to be as conservative as possible, that is, retain as much of the meniscus as possible.
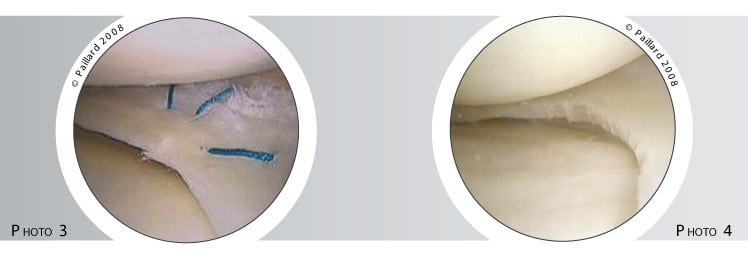
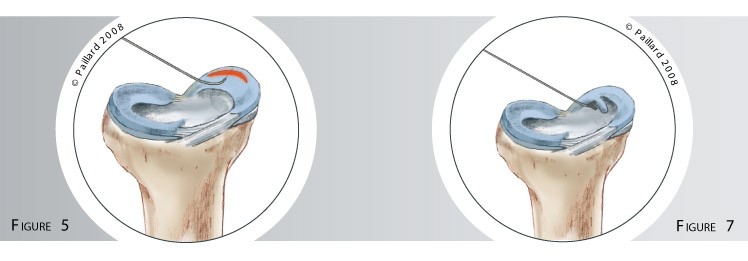
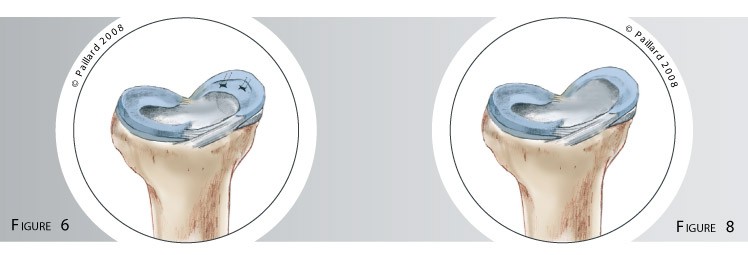
If there is a possibility of the lesion healing, the meniscus will be sutured so the entire meniscus can be retained. One or several surgical threads are passed through the lesion (figure 5) and tied together to close it (figure 6), in the same way as skin stitches, to stabilise the meniscal lesion whilst it heals (photo 3).
If the lesion has no chance of healing, the damaged part of the meniscus is removed as it is no longer functional and only causes discomfort: this is a meniscectomy. As little as possible is removed using small pliers, thus the intact part of the meniscus is retained; its complete removal is avoided where possible (figures 7 and 8, photo 4).
Cartilage damage can be treated at the same time according to its nature.
Whichever procedure is performed, the operation lasts approximately 20 to 30 minutes and is carried out as a day case: you are admitted in the morning and discharged in the evening.
The operation is carried out under regional or general anaesthesia. Your anaesthesiologist will decide with you the best type of anaesthesia according to your state of health.
After the operation, the incisions are covered with a sterile dressing, which is left in place for 10 days. The pain will be managed and monitored very closely during the post-operative period, and the treatment will be adjusted accordingly.
The post-operative procedures vary according to the operation:
In addition to the risks associated with any surgery and the anaesthetic, there are some risks specific to this surgery :
This list of risks is not exhaustive. Your surgeon can provide you with any additional explanations and will be available to discuss the advantages, disadvantages and risks of each specific case with you.
Whichever procedure is performed, the locking, swelling and feeling of instability will disappear rapidly after the operation.
The effect on the pain may depend on the existence of underlying cartilage damage. An additional medical treatment may be required.
Complete recovery of mobility and muscle strength general takes about 2 to 3 months.
After a meniscectomy, osteoarthritis can develop in the long-term according to the extent of the initial meniscal damage.
Regarding meniscal suturing, healing is not always obtained. The discomfort can thus reappear and require another arthroscopy to resect the unhealed part of the meniscus.
The results are however encouraging as the chances of healing are around 60 % for a medial meniscus and 75 % for a lateral meniscus.
Laissez votre commentaire