Biceps surgery
You have a damaged biceps at the shoulder
You are going to undergo biceps surgery
You have a damaged biceps at the shoulder
You are going to undergo biceps surgery
Biceps surgery
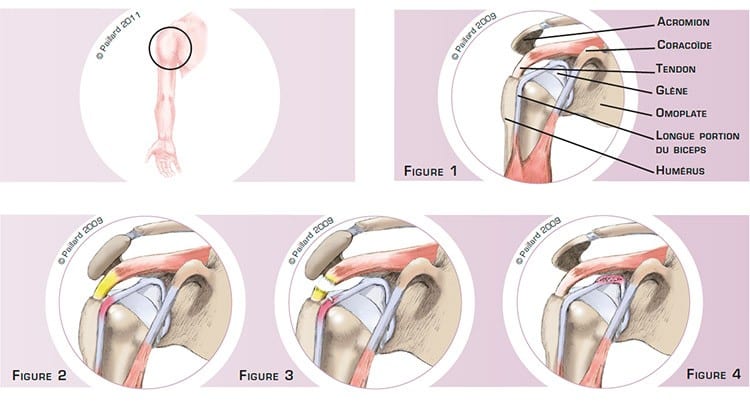
The shoulder is the joint between the scapula and the humerus. The superior part of the humerus comprises a head that pivots in the glenoid cavity of the scapula. The acromion is part of the scapula that forms an arch above the joint. The rotator cuff tendons connect the muscles to the bone. The tendons are attached to the head of the humerus and slide between the head and the acromion during lifting of the arm and rotation of the shoulder. The biceps is attached to the scapula by two tendons. The first, which is by far the biggest, is attached to the coracoid, a small bony projection on the scapular. The second, smaller and called the long head of the biceps, slides in the bicipital groove of the humerus, passes over the humeral head and is attached to the upper part of the glenoid cavity (figure 1).
A thick, curved acromion sometimes forms a bone spur, which reduces the sliding space and irritates the tendons. This results in the inflammation of the rotator cuff tendons and the long head of the biceps where it passes over the head of the humerus (figure 2). We thus talk of biceps tendonitis with subacromial impingement. The progression can lead to the rupture of the tendon (figure 3). We then talk of biceps tendonitis with rotator cuff rupture.
A biceps tendon can also be damaged where it is attached to the glenoid cavity (figure 4). This may be due to a trauma or caused by extreme movements of the shoulder, especially when playing certain sports. We thus talk of a SLAP lesion. Biceps disorders cause pain as well as difficulty in lifting the arm, and require the heavy use of oral painkillers and anti-inflammatories or injections as well as physiotherapy.
Biceps tendonitis with subacromial impingement or rupture of the rotator cuff does not disappear naturally and a detached biceps in the case of a SLAP lesion does not heal spontaneously.
Pain that persists even with medical treatment and physiotherapy raises the question of the need for surgery.
The objective of the operation is to relieve the pain, as well as to recover joint mobility and normal use of the arm.
Biceps surgery is performed arthroscopically, that is, without opening the joint. Two or three small 5-mm incisions are made around the shoulder. An arthroscope, or small camera, is inserted through one of the incisions to view the joint. Small instruments are inserted through the other incisions to perform the surgery.
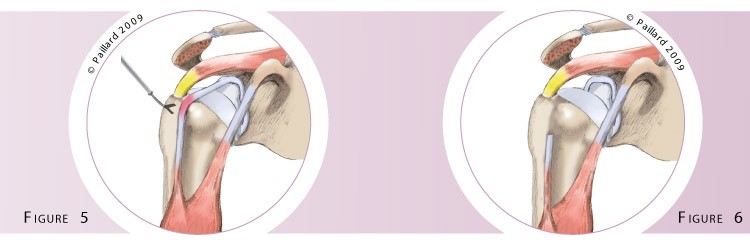
An acromioplasty, or thinning of the acromion, is systematically indicated for biceps tendonitis with subacromial impingement. It is combined with a tenotomy or a biceps tenodesis depending on the age and activity of the patient. A tenotomy consists in a single incision in the long head of the biceps (figure 5). The rest of the tendon falls down and heals in the groove (figure 6).
A tenodesis consists in fixing the tendon to the humerus and removing the intra-articular part. An anchor is screwed into the groove and the sutures from these anchors are then used to tie the tendon to the bone (figure 7).
In the case of tendonitis associated with a rotator cuff tear, the tendons are generally repaired at the same time as the tenotomy or tenodesis, except if it is a major rupture that cannot be repaired (figure 8).

In the case of a SLAP lesion, a tenotomy or a tenodesis can be proposed depending on the patient’s age and activity. A reattachment of the biceps to the glenoid cavity can be envisaged if it is a recent trauma. Two anchors are fitted to the glenoid cavity and the sutures on these anchors are then used to attach the tendon to the bone (figures 9 and 10).

Depending on the procedure, the operation lasts 30 to 60 minutes, and requires about 2 days in hospital.
The operation is carried out under regional or general anaestheia. Your anaesthesiologist will decide with you the best type of anaesthesia according to your state of health.
After the operation, the incisions are covered with a sterile dressing, which is left in place for 10 days. The pain will be managed and monitored very closely during the post-operative period, and the treatment will be adjusted accordingly. You will wear a brace to immobilize and protect your shoulder.
In the case of a simple tenotomy, you will abandon the brace within a few days. The rehabilitation, which consists in recovering shoulder flexibility and coordination, will take place at your physiotherapist’s.
Driving can be envisaged after about 15 days and you can generally return to work during the 2nd month, depending on your profession; office work can be sooner.
It should be possible to resume sports activities that do not put any strain on the shoulder during the 2nd month. You will have to wait until 4 months post-op before a full return to sports, particularly those that put strain on the shoulder.
In the case of tenodesis, reattachment or repair of the rotator cuff tendons, your shoulder will be immobilized in a shoulder immobilizer sling for 6 weeks. After the 6th week and the check-up with your surgeon, you will be able to remove the sling definitively and start rehabilitation.
It is often necessary to wait for two months before driving again and you can generally return to work during the 3rd month, depending on your profession; office work can be sooner.
A return to sports activities that do not put any strain on the shoulder can be envisaged during the 3rd month. You will have to wait until 6 months post-op before a full return to sports, particularly those that put strain on the shoulder.
In addition to the risks associated with any surgery and the anaesthetic, there are some risks specific to this surgery :
This list of risks is not exhaustive. Your surgeon can provide you with any additional explanations and will be available to discuss the advantages, disadvantages and risks of the operation with you.
In the case of tendonitis associated with subacromial impingement or rotator cuff rupture, the disappearance of the pain, an improvement in function as well as patient satisfaction is observed in around 85 % of cases for the procedures proposed.
In the case of a SLAP lesion, the reattachment of the biceps produces good results with a return to sports activities in over 90 % of cases when it is a recent post-traumatic lesion. Otherwise, a tenotomy or a tenodesis is preferred, which produces similar results.
Laissez votre commentaire