Achilles tendon repair
You have a ruptured achilles tendon
You are going to undergo achilles tendon repair

You have a ruptured achilles tendon
You are going to undergo achilles tendon repair
Achilles tendon repair
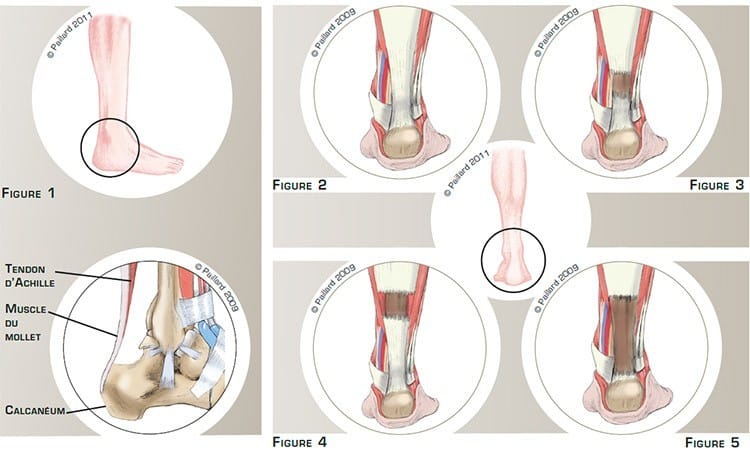
The Achilles tendon connects the calf muscle to the calcaneus, which is the heel bone (figures 1 and 2). It is a sort of rope made up of numerous filaments that extends the muscle. To stand on tiptoe, the calf muscles contract and shorten. The tendon exerts upward traction and lifts the heel off the ground.
With time or during repeated stress, the filaments of the tendon can weaken and the tendon can suddenly rupture during effort. We thus talk of Achilles tendon rupture.
There are two types of rupture: recent, or fresh, and old ruptures that were unnoticed, neglected or poorly treated.
With fresh ruptures, there are ruptures in the middle of the tendon (figure 3) and ruptures at the myotendinous junction where the muscle is connected to the tendon (figure 4).
With old ruptures, the muscle retracts and the edges are progressively resorbed, creating a space between the edges of the rupture with a loss of tendon substance (figure 5).
The tendon rupture will result in difficulty in walking, pain and a decrease in strength.
The spontaneous progression is the gradual broadening of the rupture, resulting in greater discomfort, a tendon that is more difficult to repair and therefore a more uncertain result.
Orthopaedic treatment, that is, immobilization in a plaster cast for two and a half months, is possible. However, the risk of another rupture is high.
Surgery can be proposed for active or sporty patients, thus reducing the time immobilized, speeding up recovery and reducing the rate of relapse.
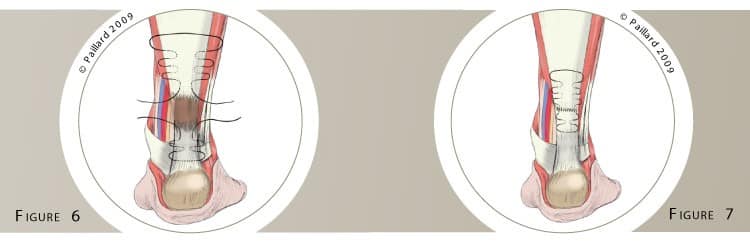
In the case of a fresh rupture in the centre of the tendon, a simple repair of the tendon is carried out.
A small surgical approach of a few centimetres is centred on the lesion. Threads are passed through each end of the tendon where it has ruptured (figure 6) to bring the two edges together and solidly repair the tendon. Additional sutures will harmonise the contact between the edges (figure 7).
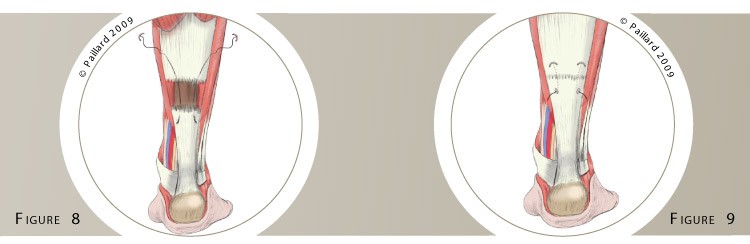
In the case of a fresh lesion in the myotendinous zone, the Tenolig system is used to restore contact between the muscle and the tendon.
This procedure is carried out percutaneously, that is, through small incisions of a few millimetres. Two threads, each connected to a harpoon, are passed through the muscle then through the gap and finally through the tendon and out through the skin (figure 8).
The threads are then stretched, the harpoons are anchored in the muscle and the ends are brought closer together (figure 9). At the end of the operation, the threads are tied together and blocked on the skin using pellets.
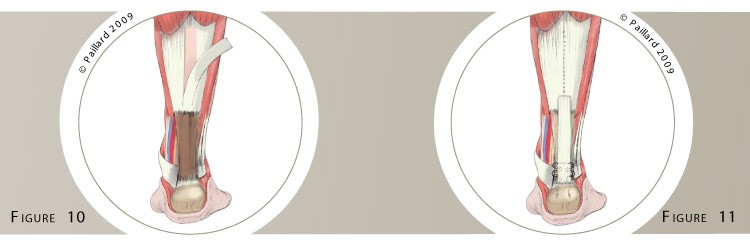
In the case of an old rupture, tendon reconstruction surgery is necessary to fill in the zone where there is a loss of tendon substance between the edges.
A longer surgical approach is thus necessary. A strip of tendon is harvested above the lesion and pulled down (figure 10). It is then solidly sutured to the lower edge using threads (figure 11). The harvesting site is closed at the end of the operation, and will heal and get stronger with time.
The operation lasts about 1 hour, and requires around 3 days in hospital. The operation can be carried out under spinal or general anaesthesia. Your anaesthesiologist will decide with you the best type of anaesthesia according to your state of health.
After the operation, your foot will be put in a brace then a resin cast. The pain will be managed and monitored very closely during the post-operative period, and the treatment will be adjusted accordingly.
You will wear the resin cast for 6 weeks. You will have crutches to help you move around throughout this period, putting no weight on your foot.
When the cast is removed, you will walk with a heelpiece of which the thickness is progressively decreased over 3 weeks. The rehabilitation will then begin at your physiotherapist’s. Normal walking is recovered at the end of the 2nd month.
Driving and returning to work can be envisaged in the 3rd month, depending on your profession; office work can be sooner.
You can resume gentle sports activities like cycling and swimming after the 3rd month. Running can be envisaged after the 6th month. It may be necessary to wait until the 8th month before a return to team sports and competition.
In addition to the risks associated with any surgery and the anaesthetic, there are some risks specific to this surgery :
This list of risks is not exhaustive. Your surgeon can provide you with any additional explanations and will be available to discuss the advantages, disadvantages and risks of each specific case with you.
In the context of a fresh rupture, the rate of tendon healing is over 95 %. The tendon is sometimes thicker. The risk of another rupture is below 5 %.
In the case of an old rupture, the rate of healing is pretty much the same but takes longer, thus delaying the return to activities.
The results of surgical repair of the Achilles tendon are nevertheless very encouraging as in over 90 % of cases patients return to sports activities at their previous level.
Laissez votre commentaire