Acromioclavicular stabilization
You have an acromioclavicular luxation
You are going to undergo acromioclavicular stabilization
You have an acromioclavicular luxation
You are going to undergo acromioclavicular stabilization
Acromioclavicular stabilization
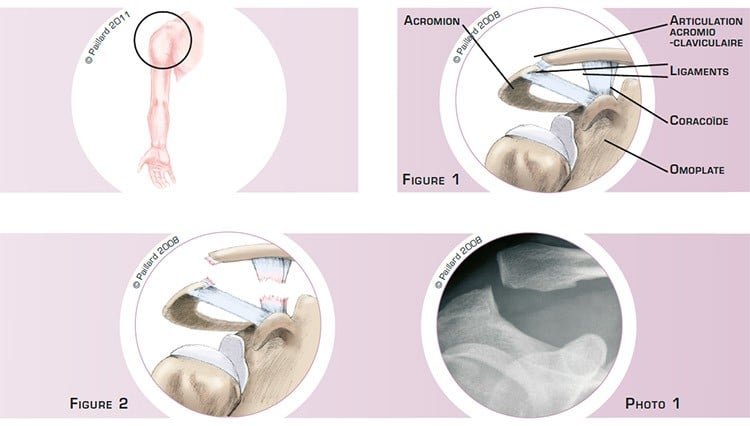
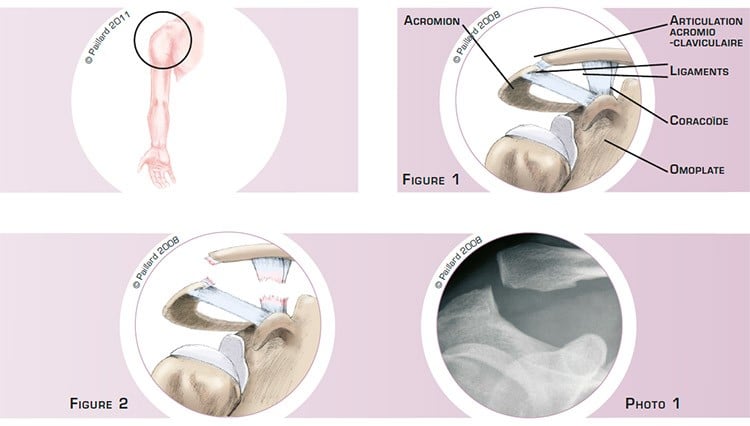
The scapular comprises several bony parts, in particular the acromion, which is the part at the top of the shoulder blade, and the coracoid process, which is a bony projection at the front of the shoulder blade (figure 1).
The acromioclavicular joint connects the acromion to the collarbone and is held in place by several ligaments that are like ribbons of varying elasticity. The acromioclavicular ligaments surround the joint, and the coracoclavicular ligaments, which are not in contact with the joint, connect the coracoid to the collarbone (figure 1).
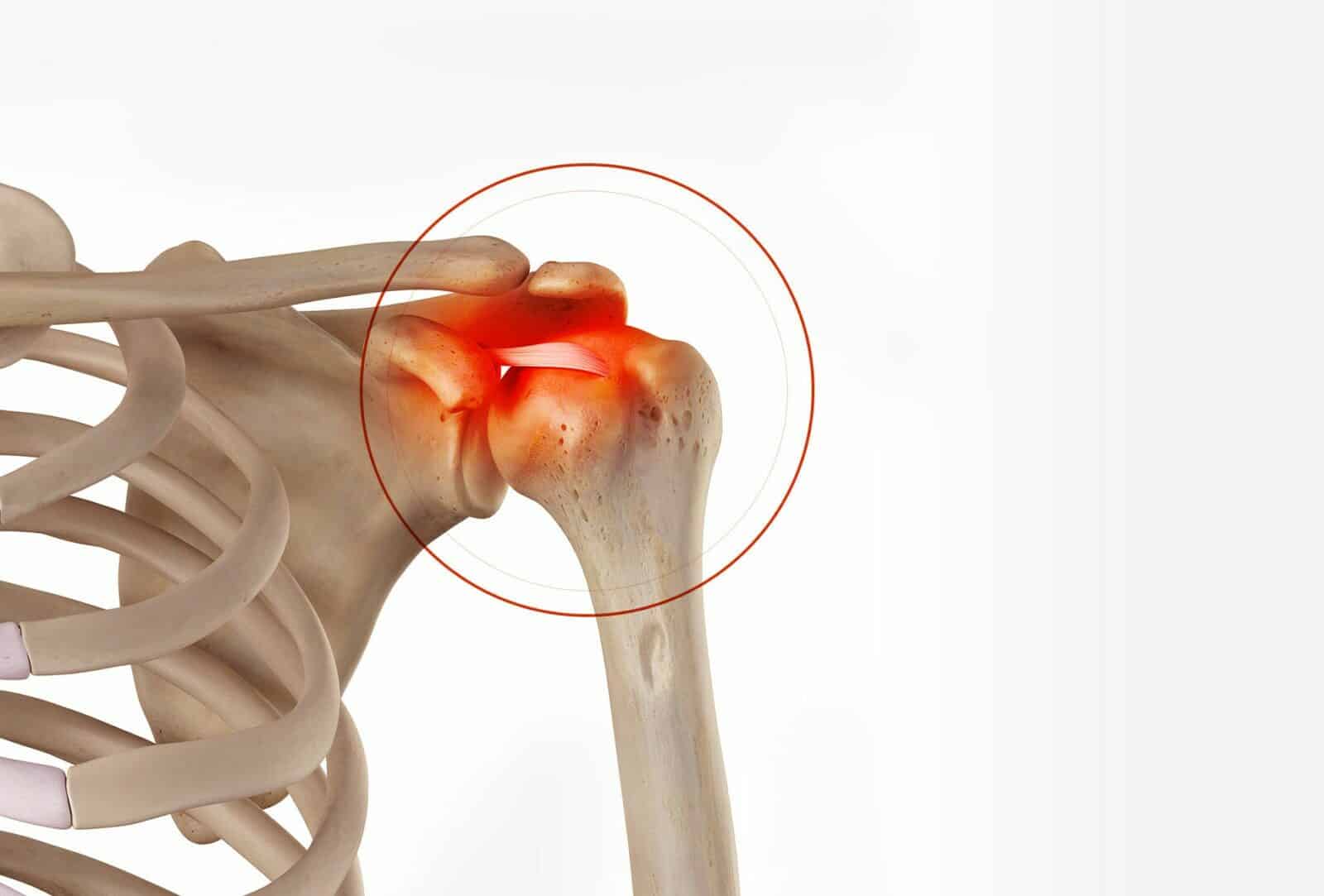
A trauma to the shoulder can cause the rupture of these ligaments, so they no longer hold the acromioclavicular joint together. Gravity pulls the shoulder and the scapula downwards and the muscles pull the collarbone upwards (figure 2 and photo 1). We thus talk of acromioclavicular luxation that can result in fatigability, pain and a visible deformation.
An acromioclavicular luxation does not resolve itself spontaneously, and in the absence of a surgical procedure the collarbone remains ascended. Furthermore, the ligaments do not heal in an effective position and so the collarbone is not held in place.
This high position of the collarbone, apart from the aesthetic inconvenience, can cause permanent discomfort and fatigability when carrying out daily activities or sports.
The aim of acromioclavicular stabilization is to restore the collarbone to its correct position and recover optimal shoulder function, thus enabling a return to all activities without discomfort.
Acromioclavicular stabilization consists in durably repositioning the collarbone in its natural position. The procedure is performed arthroscopically or through a small incision at the front of the shoulder. An arthroscopy consists in making two or three small 5-mm incisions around the shoulder. An arthroscope, or small camera, is inserted through one of the incisions for viewing and small instruments are inserted through the other incisions to perform the surgery.
If the surgery is carried out rapidly after the trauma, the collarbone only needs to be returned to its natural position. The ruptured ligaments can then heal in the right position and durably hold the collarbone in place. This is a “simple stabilization”, and is often carried out arthroscopically. The principle is to lower the collarbone and attach it to the coracoid using a system of resistant threads, which are tied together, thus holding the collarbone in place so the ligaments can heal effectively (figures 3 and 4, photo 2).

If the surgery is performed some time after the trauma, the ligaments will no longer have the ability to heal. It will therefore be necessary to reposition the collarbone and replace the ruptured ligaments with a new ligament; this is “ligament reconstruction”. It often requires a short incision in the front of the shoulder, but can sometimes be performed arthroscopically. In addition to a simple stabilization with a system of resistant threads between the collarbone and the coracoid, the ligaments are replaced. To do so, the extremity of the collarbone is cut (figure 5). The arcomioclavicular ligament, which is an accessory ligament stretched between the coracoid and the acromion, is detached from the latter. It is then fixed in the cut made in the collarbone, thus replacing the ruptured ligaments (figure 6, photo 3).

Whichever technique is used, the operation lasts about 1 hour and requires 2 days in hospital.
The operation is carried out under regional or general anaesthesia. Your anaesthesiologist will decide with you the best type of anaesthesia according to your state of health.
After the operation, the incisions are covered with a sterile dressing, which is left in place for 10 days. The pain will be managed and monitored very closely during the post-operative period, and the treatment will be adjusted accordingly. You will wear a shoulder immobilizer sling to immobilize and protect your shoulder.
During the first 6 weeks post-op you will wear a shoulder immobilizer sling to immobilize your shoulder. After the 6th week and the check-up with your surgeon, you will be able to remove the sling definitively and start rehabilitation, which consists in recovering shoulder flexibility, strength and coordination.
It is often necessary to wait until the 2nd month before driving again. You can generally return to work between the 2nd and the 3rd month, depending on your profession. If you work in an office, you may be able to return to work sooner after the operation.
You can envisage resuming sports activities that do not put any strain on the shoulder after the 2nd month. In the case of a simple stabilization, you will have to wait until the 4th month post-op before a full return to sports, particularly those that put strain on the shoulder. You will have to wait 6 months in the case of ligament reconstruction.
In addition to the risks associated with any surgery and the anaesthetic, there are some risks specific to this surgery :
This list of risks is not exhaustive. Your surgeon can provide you with any additional explanations and will be available to discuss the advantages, disadvantages and risks of each specific case with you.
The deformation, pain and fatigability will disappear rapidly after the operation. Complete recovery of mobility and muscle strength generally takes about 2 to 3 months.
The healed ligaments and the replaced ligament are no better than the original ligaments and can rupture again following a trauma. Ligament distension or even osteoarthritis of the acromioclavicular joint can also develop.
The results of this surgery are nevertheless very encouraging as a stable joint with a disappearance of the pain and a return to all activities is observed in over 90 % of cases.
Laissez votre commentaire