Hip arthroscopy
You have an intra-articular pathology of the hip
You are going to undergo a hip arthroscopye

You have an intra-articular pathology of the hip
You are going to undergo a hip arthroscopye
Hip arthroscopy
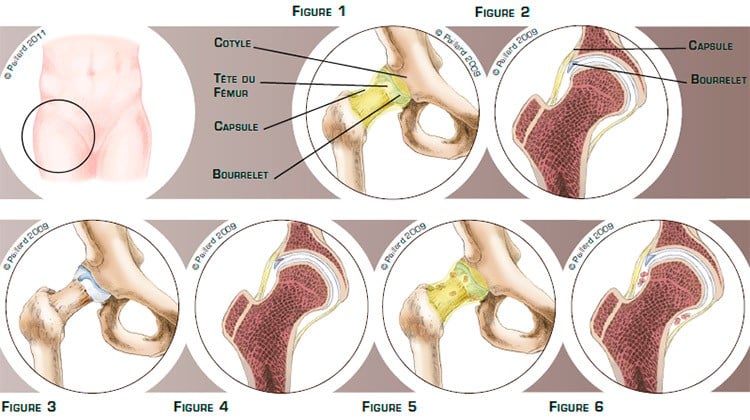
The hip is the joint between the pelvis and the femur. The top of the femur is composed of a head and a neck, which pivots in a socket in the pelvis called the acetabulum, and the sliding surfaces are lined with cartilage. The labrum is a sort of C-shaped cushion, which improves the contact and acts as a shock absorber between the cartilage of the femoral head and the acetabulum. The joint capsule lined with the synovial membrane is a sort of sealed envelope which surrounds and stabilises the joint. Numerous muscles and tendons surround the capsule and ensure hip mobility and a balanced gait (figures 1 and 2).
An intra-articular pathology of the hip is damage inside the joint capsule. The two most common pathologies are labral damage and intra-articular foreign bodies.
Labral damage can occur following a blow to the hip or recurrent minor traumas suffered during certain movements. This lesion can affect the labrum to a varying extent. It can be stable, or unstable in the form of a bell clapper which moves in the joint (figures 3 and 4).
An intra-articular foreign body comes from a detached cartilage lesion or is formed by the synovial membrane and released inside the joint (figures 5 and 6).
These lesions cause pain, locking and sometimes stiffness and difficulty in walking, and can require the use of anti-inflammatories, painkillers and sometimes even a walking stick.
Labral damage or an intra-articular foreign body does not heal spontaneously. The foreign bodies can become imprisoned between the acetabulum and the head of the femur and damage the cartilage. The pain can initially be treated medically.
However, surgery will be proposed in the case of intra-articular locking sensations or pain that is not relieved by the medical treatment.The aim of the operation is to relieve the pain and locking, protect the surfaces of the joint in the case of foreign bodies, and return to normal walking and activities.
A hip arthroscopy enables the hip to be accessed without opening the joint, sparing the anatomical structures, in particular the muscles. This technique therefore has proven advantages in relation to traditional surgery, including minimal blood loss and faster post-operative recovery.
The technique consists in making two small 5-mm incisions around the hip.
Your leg will be put in traction to create a space to work inside the joint. An arthroscope, or small camera, is inserted through one of the incisions to view the joint, in particular the damaged labrum or the intra-articular foreign bodies. Small instruments are inserted through the other incisions to carry out the surgery.

If the labrum is damaged,
the damaged part is removed as it is no longer functional and only causes discomfort. As little as possible is removed using small pliers. The intact part of the labrum is retained; its complete removal is avoided where possible (figures 7, 8, 9 and 10).

In the case of an excessive angle of the femoral neck and an insufficient covering of the acetabulum,
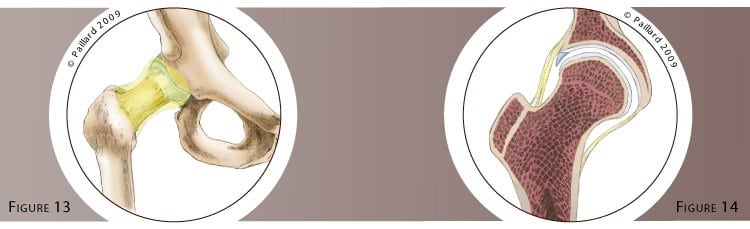
In the case of intra-articular foreign bodies, a hip lavage is carried out first. Large foreign bodies are identified then removed using arthroscopic pliers. Small foreign bodies are removed using a small vacuum cleaner (figures 11, 12, 13 and 14).
Associated cartilage damage can be treated at the same time according to its nature.
Whichever procedure is used, the operation lasts approximately one hour and requires two or three days in hospital.
The operation is carried out under spinal or general anaesthesia. Your anaesthesiologist will decide with you the best type of anaesthesia according to your state of health.
After the operation, the incisions are covered with a sterile dressing, which is left in place for 10 days. The pain will be managed and monitored very closely during the post-operative period, and the treatment will be adjusted accordingly.
The day after the operation, the physiotherapist will get you up and help you to walk. Walking sticks will be useful during the first few days, but will be rapidly abandoned.
It is not necessary to go to a rehabilitation centre or to a physiotherapist’s after your stay in hospital. Progressively resuming your activities will be your physiotherapy.
Driving can be envisaged rapidly after a few days, and you can generally return to work after the 1st month, depending on your profession; office work can be sooner. You can progressively resume sports activities after the 2nd month, but it is often necessary to wait until the 4th month to return to competition.
In addition to the risks associated with any surgery and the anaesthetic, there are some risks specific to this surgery :
This list of risks is not exhaustive. Your surgeon can provide you with any additional explanations and will be available to discuss the advantages, disadvantages and risks of the operation with you.
Whatever the initial pathology, the locking will disappear rapidly after the operation.
Normal walking without limping is generally recovered within the 1st month.
The effect on the pain may depend on the existence of underlying cartilage damage. An additional medical treatment may be required.
In the absence of cartilage damage, the results are satisfactory in over 90 % of cases and the risk of relapse remains extremely minimal.
Laissez votre commentaire