Unicompartmental knee replacement
You have unicompartmental osteoarthritis of the knee
You are going to undergo a unicompartmental knee replacement

You have unicompartmental osteoarthritis of the knee
You are going to undergo a unicompartmental knee replacement
Unicompartmental knee replacement
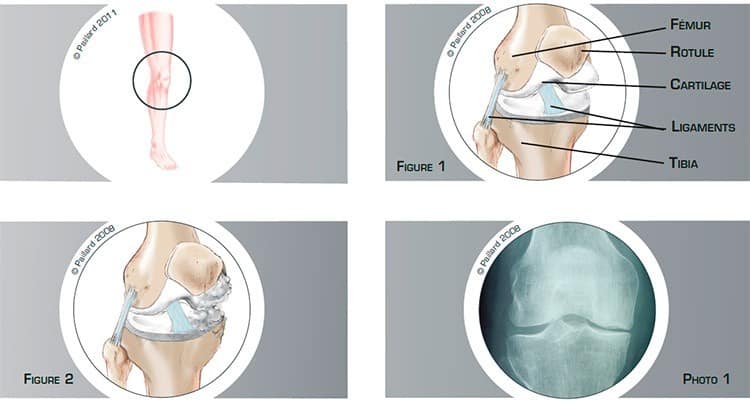
The knee is the joint between the femur and the tibia. The patella is the third bony part of the joint and is located in front. The sliding surfaces are lined with cartilage (figure 1), and numerous muscles and tendons surrounding the joint enable bending and straightening of the knee. The ligaments, which are ribbons of varying elasticity, help maintain the stability of the knee. Osteoarthritis is the wear and tear of the cartilage on the sliding surfaces. This wear and tear is also accompanied by a modification of the underlying bone, which can affect all or just part of the knee (figure 2 and photo 1).
These modifications cause pain in the knee as well as stiffness and difficulty in walking, and require the use of anti-inflammatories, painkillers and sometimes a walking stick.
The wear of the cartilage is irreversible and osteoarthritis does not heal spontaneously. The natural progression is the gradual deterioration of the joint, increasingly limited mobility and increased difficulty in walking.
The anti-inflammatories and painkillers that were enough to start with are no longer effective, and so the question of surgery is raised.
The objective of the operation is to relieve the pain, recover joint mobility and return to normal walking.
The objective of a knee replacement is to remove the areas of bone and cartilage that are worn, and to replace them with artificial parts of the same shape. When the wear affects the entire knee, total replacement is proposed. When the wear only affects part of the knee, a unicompartmental knee replacement is indicated. The advantage is to preserve the natural parts of the knee that are not worn and only replace the damaged part. This procedure is performed using a minimally invasive technique, causing as little damage as possible to the muscles and tendons around the knee. This technique has advantages in relation to traditional surgery, including faster post-operative recovery.
An incision is made in the anterior part of the knee.
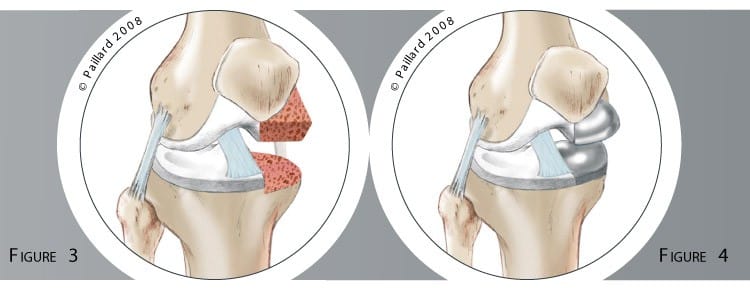
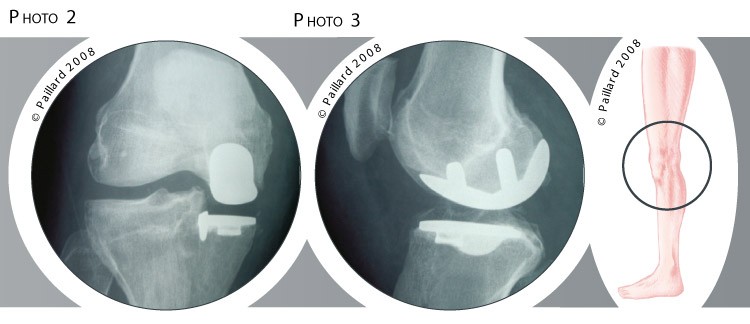
A passage is created behind the patella to access the joint and the worn cartilage is removed. The healthy cartilage and all the ligaments are retained. The worn part of the femur and the worn part of the tibia are prepared (figure 3). The prosthesis, made up of a femoral component and a tibial component, is then fitted to ensure the perfect stability and greatest possible mobility of the knee (figure 4, photos 2 and 3).
Computer-aided techniques can be used to control the correct positioning.
The operation lasts about 1 hour on average and requires around 5 days in hospital.
Unicompartmental knee replacement is carried out under spinal or general anaesthesia. Your anaesthesiologist will decide with you the best type of anaesthesia according to your state of health. After the operation, the incisions are covered with a sterile dressing, which is left in place for 15 days. The pain will be managed and monitored very closely during the post-operative period, and the treatment will be adjusted accordingly. A brace will be used to immobilize and protect your knee during the first few days.
The day after the operation, the physiotherapist will get you up and help you to walk. Walking sticks will be useful during the first few days, but will be rapidly abandoned. You can go up and down stairs within 3 days. Except for very specific cases, it is not necessary to go to a rehabilitation centre. The rehabilitation is generally carried out by your physiotherapist. Driving can be envisaged after the 1st month and you can generally return to work after the 2nd month, depending on your profession; office work can be sooner. You can progressively resume sports activities after the 3rd month.
In addition to the risks associated with any surgery and the anaesthetic, there are some risks specific to this surgery :
This list of risks is not exhaustive. Your surgeon can provide you with any additional explanations and will be available to discuss the advantages, disadvantages and risks of each specific case with you.
The results of this technique are very encouraging as an often spectacular disappearance of the pain along with a rapid recovery of mobility and muscle strength are observed. Normal walking with no limping is generally recovered within one month post-op.
Even if the return to activities is often unrestricted, it is preferable to avoid physical work and violent sports as these activities can increase the wear and decrease the lifespan of the prosthesis despite the use of new, more resistant materials. Some activities like cycling, swimming, golf or walking are possible, and even recommended, whereas care should be taken with skiing, tennis and jogging.
The average lifespan of a knee replacement is about 15 years. With the progress in the materials used today, and the computer-assisted positioning of the implants, we hope that the results and the longevity will continue to improve.
Laissez votre commentaire