Ankle ligament reconstruction
You have ankle instability
You are going to undergo ankle ligament reconstruction

You have ankle instability
You are going to undergo ankle ligament reconstruction
Ankle ligament reconstruction
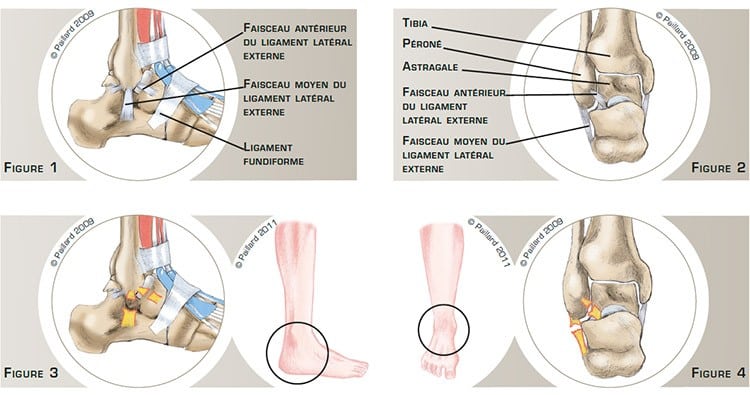
The ankle is the joint between the bottom of the tibia and the fibula and the upper part of the talus, which is the first bone in the foot located just above the calcaneus. The sliding surfaces are lined with cartilage.
The ligaments are ribbons of varying elasticity that help maintain the stability of the ankle. The external lateral ligaments are located on the lateral side of the ankle and connect the fibula to the talus and the calcaneus. There are three ligaments that prevent the ankle and the foot twisting inwards: the anterior and posterior talofibular ligaments, which connect the fibula to the talus, and the calcaneofibular ligament, which stretches between the fibula and the calcaneus (figure 1 and 2).
The anterior talofibular and calcaneofibular ligaments of the external lateral ligaments are more often affected during a trauma (figures 3 and 4). They can be simply distended or completely ruptured, resulting in ankle swelling and pain. We thus talk of a sprained ankle, which can be more or less serious and require immobilization for the ligament to heal. Recurrent sprains reduce the capacity of the ligament to heal spontaneously in an effective position, thus decreasing the stability of the ankle. We thus talk of ankle instability responsible for pain and feelings of giving way.
Some sports or daily activities are impossible in the absence of effective external lateral ligaments, and can lead to instability accidents and cause cartilage damage. In this context, the natural progression is the gradual deterioration of the joint.
The objective of the reconstruction is to recover a perfectly stable ankle to be able to carry out all types of activities, thus preventing cartilage damage and the deterioration of the joint.
Ankle ligament reconstruction consists in reconstructing the anterior talofibular ligament and the calcaneofibular ligament of the external lateral ligament.
An incision is made on the lateral side of the ankle.
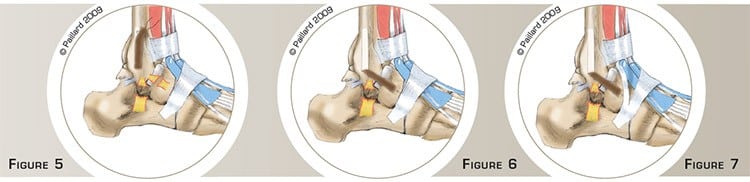
A strip of periosteum, which is the membrane covering the bone, is harvested on the fibula. It is pulled down and inserted in the tip of the fibula at the proximal insertion of the anterior talofibular ligament (figure 5). An anchor is screwed to the talus at the insertion of the distal end of this ligament. The threads on the anchor are passed through the free end of the strip and tied together to fix it to the bone. This reconstructs the anterior ligament of the external lateral ligaments (figure 6).
Part of the extensor retinaculum, which maintains the toe tendons, is harvested.
It is turned up and inserted in the calcaneus at the distal insertion of the calcaneofibular ligament (figure 7). An anchor is screwed to the tip of the fibula at the proximal insertion of this ligament. The threads on the anchor are passed through the free end of the strip and tied together to fix it to the bone. This reconstructs the calcaneofibular ligament (figures 8 and 9).

The operation lasts about 1 hour, and requires around 3 days in hospital. This operation is carried out under regional or general anaesthesia. Your anaesthesiologist will decide with you the best type of anaesthesia according to your state of health.
After the operation, your foot will be put in a brace then a resin cast. The pain will be managed and monitored very closely during the post-operative period, and the treatment will be adjusted accordingly.
You will wear the resin cast for 6 weeks. You will have crutches to help you move around throughout this period, putting no weight on your foot.
You can put weight on your foot once the cast is removed. You will then start your rehabilitation at your physiotherapist’s. Normal walking is recovered at the end of the 2nd month.
Driving and returning to work can be envisaged in the 3rd month, depending on your profession; office work can be sooner.
You can resume gentle sports activities like cycling and swimming after the 3rd month. Running can be envisaged after the 4th month. It may be necessary to wait until the 6th month before a return to team sports and competition.
In addition to the risks associated with any surgery and the anaesthetic, there are some risks specific to this surgery :
This list of risks is not exhaustive. Your surgeon can provide you with any additional explanations and will be available to discuss the advantages, disadvantages and risks of each specific case with you.
The pain and feeling of instability should disappear very rapidly after the operation. Complete recovery of mobility and muscle strength generally takes about 3 to 6 months.
The condition of the muscles is a major element to be taken into consideration before pushing the ankle to the limit, in particular in sport. The replaced ligament is no better than the original ligament and can rupture again. It is therefore necessary to be careful given the risks posed by sports that put strain on the ankle.
The results of this technique are nevertheless very encouraging as a stable ankle with improved function is recovered in over 90 % of cases. A stable ankle reduces the risk of cartilage deterioration.
Laissez votre commentaire