Shoulder stabilization
You have an unstable shoulder
You are going to undergo shoulder stabilization

You have an unstable shoulder
You are going to undergo shoulder stabilization
Shoulder stabilization
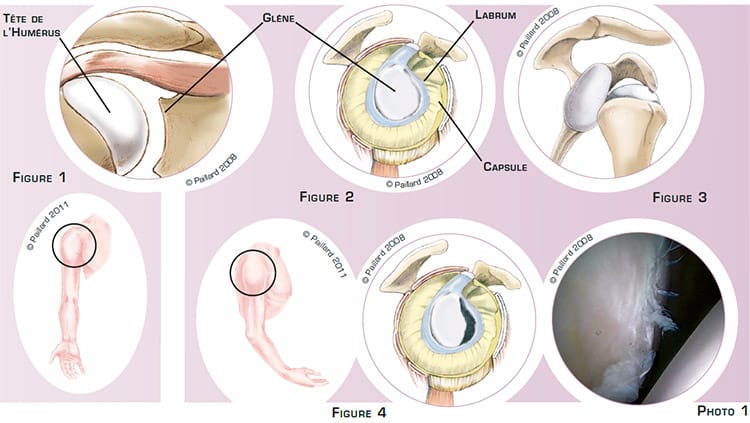
The shoulder is the joint between the scapula and the humerus. The superior part of the humerus comprises a head that pivots in the glenoid cavity of the scapula (figure 1), and the sliding surfaces are lined with cartilage. Despite this joint’s extremely broad range of motion, several structures maintain the humeral head in permanent contact with the glenoid cavity: the joint capsule, an envelope surrounding the joint, the ligaments, ribbons connecting the glenoid cavity to the humerus, and the labrum, an elastic rim around the glenoid cavity (figure 2).
Following a trauma resulting in the dislocation of the shoulder (figure 3), these structures may be stretched or ruptured (figure 4 and photo 1). In this context, the head is not held in place as well, and the shoulder can dislocate more or less completely during a sports activity or even during daily activities.
We thus talk of an unstable shoulder that can result in apprehension and pain.
Each time the head comes out of position, the damage to the stabilizing structures worsens, damaging the cartilage on the joint surfaces.
The natural progression is more frequent luxations, greater apprehension, as well as a gradual deterioration of the joint.
The aim of shoulder stabilization surgery is to prevent recurrent dislocations and thus enable a full return to activities and prevent the progressive deterioration of the joint.
Shoulder stabilization consists in preventing the head of the humerus from coming out of its natural position. There are two surgical procedures possible: the retention of the capsule and the ligaments using the Bankart procedure, or the placement of a piece of bone on the edge of the glenoid cavity using the augmentation procedure.
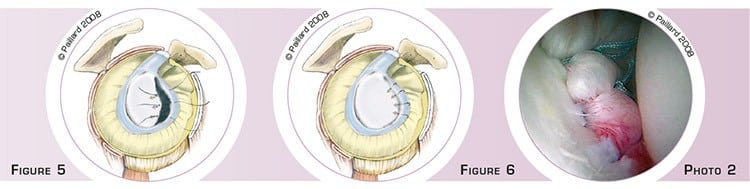
The Bankart procedure is performed arthroscopically, that is, without opening the shoulder joint. Two or three small 5-mm incisions are made around the shoulder. An arthroscope, or small camera, is inserted through one of the incisions to view the joint, and in particular the damaged capsule and the ligaments. Small instruments are inserted through the other incisions to perform the surgery. Two anchors are implanted in the glenoid cavity, the threads on the anchors are passed through the capsule and the ligaments (figure 5), and tied together in order to reattach these structures to the bone (figure 6 and photo 2).

The augmentation procedure requires a short incision in the front of the shoulder.
The coracoid, a small bony projection on the scapular, is removed. It is then fixed to the anterior edge of the glenoid cavity by one or two screws and forms an augmentation preventing the head of the humerus from dislocating (figures 7 and 8).
We prefer the Bankart arthroscopic procedure as it restores the anatomy of the shoulder and does not require the opening of the joint. However, some conditions require an augmentation, for example significant bone damage or a high-risk sports activity.
Whichever technique is used, the operation lasts about 1 hour and requires 2 days in hospital.
The operation is carried out under regional or general anaesthesia. Your anaesthesiologist will decide with you the best type of anaesthesia according to your state of health.
After the operation, the incisions are covered with a sterile dressing, which is left in place for 10 days. The pain will be managed and monitored very closely during the post-operative period, and the treatment will be adjusted accordingly. You will wear a shoulder immobilizer sling to immobilize and protect your shoulder.
During the first 4 weeks post-op, you will wear a shoulder immobilizer sling to immobilize your shoulder. After the 4th week and the check-up with your surgeon, you will be able to remove the sling definitively and start rehabilitation, which consists in recovering shoulder flexibility, strength and coordination.
It is often necessary to wait until the 2nd month before driving again. You can generally return to work between the 2nd and 3rd month, depending on your profession. If you work in an office, you may be able to return to work more rapidly after the operation.
A full return to sports activities can be envisaged after the 3rd month if you had an augmentation. In the case of arthroscopic Bankart repair, it is necessary to wait until the 6th month before resuming sports that put strain on the shoulder. It will be necessary to wait another 1 or 2 months to recover all your natural reflexes and to return to competition.
In addition to the risks associated with any surgery and the anaesthetic, there are some risks specific to this surgery :
This list of risks is not exhaustive. Your surgeon can provide you with any additional explanations and will be available to discuss the advantages, disadvantages and risks of each specific case with you.
The pain, apprehension and feeling of instability should disappear very rapidly after the operation. Complete recovery of mobility and muscle strength generally takes about 2 to 3 months.
A relapse in instability depends above all on the sport played. It is therefore necessary to be careful given the risks posed by sports that involve a wind up stage such as tennis, basketball, handball or even rugby.
The results of this technique are nevertheless very encouraging as a stable shoulder is achieved in 90 % of cases for the arthroscopic Bankart procedure and in 95 % of cases for an augmentation. The risk of cartilage deterioration is lower with a stable shoulder.
Laissez votre commentaire