Shoulder acromioplasty
You have a subacromial shoulder impingement
You are going to undergo a shoulder acromioplasty

You have a subacromial shoulder impingement
You are going to undergo a shoulder acromioplasty
Shoulder acromioplasty
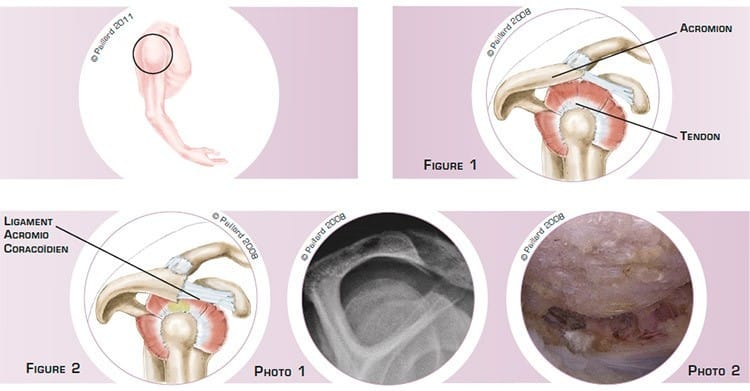
The shoulder is the joint between the scapula and the humerus. The superior part of the humerus comprises a head that pivots in the glenoid cavity of the scapula. The acromion is part of the scapula that forms an arch above the joint with the acromiocoracoid ligament. The tendons connecting the muscles to the bone are attached to the head of the humerus and slide between the head and the acromion during lifting of the arm and rotation of the shoulder (figure 1).
The acromion can be of varying thickness and more or less curved and sharp, thus reducing the sliding space for the tendons. When lifting the arm, the tendons hit and rub against the acromion, which can sometimes form a bone spur. Subacromial impingement is an excessive and recurrent contact between the tendons and the acromion, which causes inflammation of the tendons and can result in rupture (figure 2 and photos 1 and 2).
Subacromial impingement causes pain and can even result in a decrease in shoulder mobility as well as difficulty in lifting the arm; this can require the heavy use of oral painkillers and anti-inflammatories or injections as well as physiotherapy.
Subacromial impingement does not disappear spontaneously, and it sustains the inflammation of the tendons. In these conditions, the natural progression is a gradual weakening of the tendons until rupture and therefore increased discomfort.
Pain that persists with the medical treatment and physiotherapy raises the question of the need for surgery.
The aim of the operation is to relieve the pain, as well as recover mobility and normal use of the arm, thus preventing the deterioration and ultimately the rupture of the tendons.
An acromioplasty aims to remove the impingement by increasing the sliding space for the shoulder tendons. This procedure is performed arthroscopically, that is, without opening the joint. Arthroscopy spares the anatomical structure and the joint can be accessed without damaging the muscles. This technique therefore has proven advantages in relation to traditional surgery, including minimal blood loss and faster post-operative recovery.
Two or three small 5-mm incisions are made around the shoulder. An arthroscope, or small camera, is inserted through one of the incisions to view the joint, and in particular the area where the tendon rubs against the bone. Small instruments are inserted through the other incisions to perform the surgery.
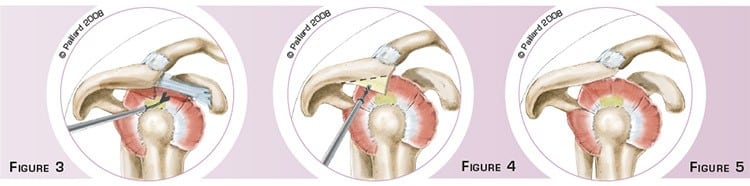
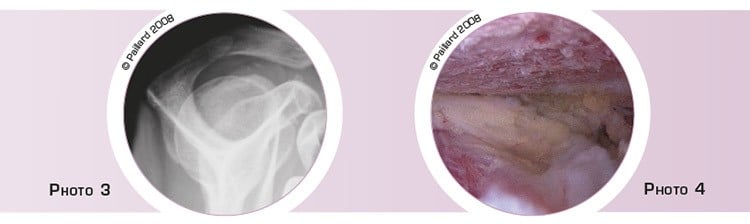
Firstly the shoulder is cleaned and the inflamed tissue is resected. The acromion bone and the acromioclavicular ligament are then freed and exposed. The arcomioclavicular ligament, which is an accessory ligament stretched between the coracoid and the acromion, is detached from the latter (figure 3). The aggressive part of the acromion responsible for the impingement is marked then resected using a motorised cutter that cuts the bone and sucks up the debris (figure 4). The acromion is therefore progressively thinned and the bone spur completely removed. At the end of the operation, we check that it is completely flat, that the tendons have enough space during movement and that the impingement has been removed (figure 5, photos 3 and 4).
In the case of a ruptured tendon undiagnosed during the pre-operative assessment and discovered during the operation, the tendon is repaired at the same time.
The operation lasts about half an hour on average, and requires about 2 days in hospital.
The acromioplasty is carried out under regional or general anaesthesia. Your anaesthesiologist will decide with you the best type of anaesthesia according to your state of health.
After the operation, the incisions are covered with a sterile dressing, which is left in place for 10 days. The pain will be managed and monitored very closely during the post-operative period, and the treatment will be adjusted accordingly. You will wear a brace to immobilize and protect your shoulder.
The day after the operation, the physiotherapist will help you move your shoulder. Within a few days, you will no longer need the brace. The rehabilitation, which consists in recovering shoulder flexibility and coordination, will take place at your physiotherapist’s.
Driving can be envisaged after about 15 days, and you can generally return to work during the 2nd month, depending on your profession; office work can be sooner.
A return to sports activities that do not put any strain on the shoulder can be envisaged during the 2nd month. You will have to wait until 4 months post-op before a full return to sports, particularly those that put strain on the shoulder.
In addition to the risks associated with any surgery and the anaesthetic, there are some risks specific to this surgery :
This list of risks is not exhaustive. Your surgeon can provide you with any additional explanations and will be available to discuss the advantages, disadvantages and risks of each specific case with you.
The final outcome depends above all on the duration of the pain and the state of the tendons. Long-term pain with damaged tendons produces poorer results.
The time the pain takes to disappear varies. Complete recovery generally takes about 3 to 6 months.
The results of this surgery are however very encouraging as patient satisfaction is observed in over 85 % of cases. The improvement concerns the pain and shoulder function. These results are maintained over time and it is only necessary to operate on the tendons in less than 10 % of cases after 25 years.
Laissez votre commentaire